
Overcoming the Sigma – Part 3
The convoluted or twisted sigmoid

Fig. 1: Radiologic appearance of the twisted sigmoid colon
The category of “twisted” sigmoid includes a number of conditions where the anatomy of the sigmoid escapes typical morphologies, either because of postoperative adhesions or because of an unusually long colonic segment, with the meso-sigmoid not necessarily elongated (fig. 1). In this case, the ascending branch of the sigmoid (ᔐ-top) has a more or less regular arched shape, while the descending branch (ᔐ-down) has a very variable shape, showing several sequential loops before conjoining the sigmoid-descending junction (fig. 2).

Fig. 2: In the twisted sigmoid, the ascending branch has a regular, arched shape (green arrow), while the descending branch (yellow arrow) shows several sequential loops before conjoining to the sigmoido-descending junction (RS-J); some of these lops can be mobilized with the tip of the scope, while others can sometimes be fixed due to adhesions.
The most favorable position to pass this type of sigmoid is the supine position (fig. 3); the compression on the abdomen is very useful and should be performed gently with two fingers directly by the endoscopist, searching for the area where it helps the progression of the tip.

Fig. 3: the best position to pass a twisted sigmoid is the supine position, taking maximum advantage from the manual abdominal compression.
In patients with a twisted sigmoid, after passing of the descending branch of the colonic segment, the endoscopist comes across a series of sequential loops, one next to the other, requiring a centimeter-by centimeter progression with continuous alternate right- and left-torques to keep the axis of the lumen.
Also in this situation, the essential rule is to keep the shaft of the scope as straight as possible and achieve the progression moving the tip as in a “slalom” hooking with the tip deflection each fold encountered (‘cork-screw twist insertion’ – fig. 4 A-D)

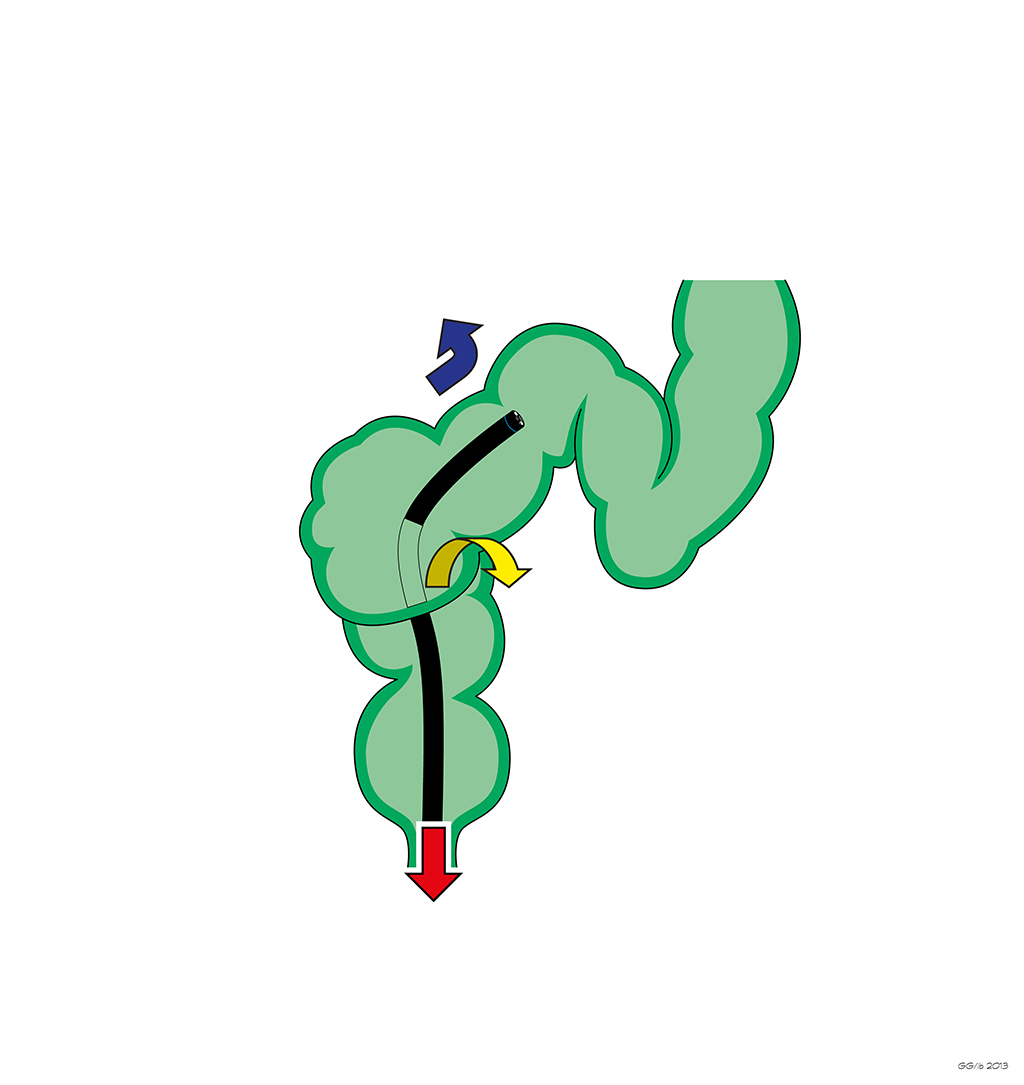
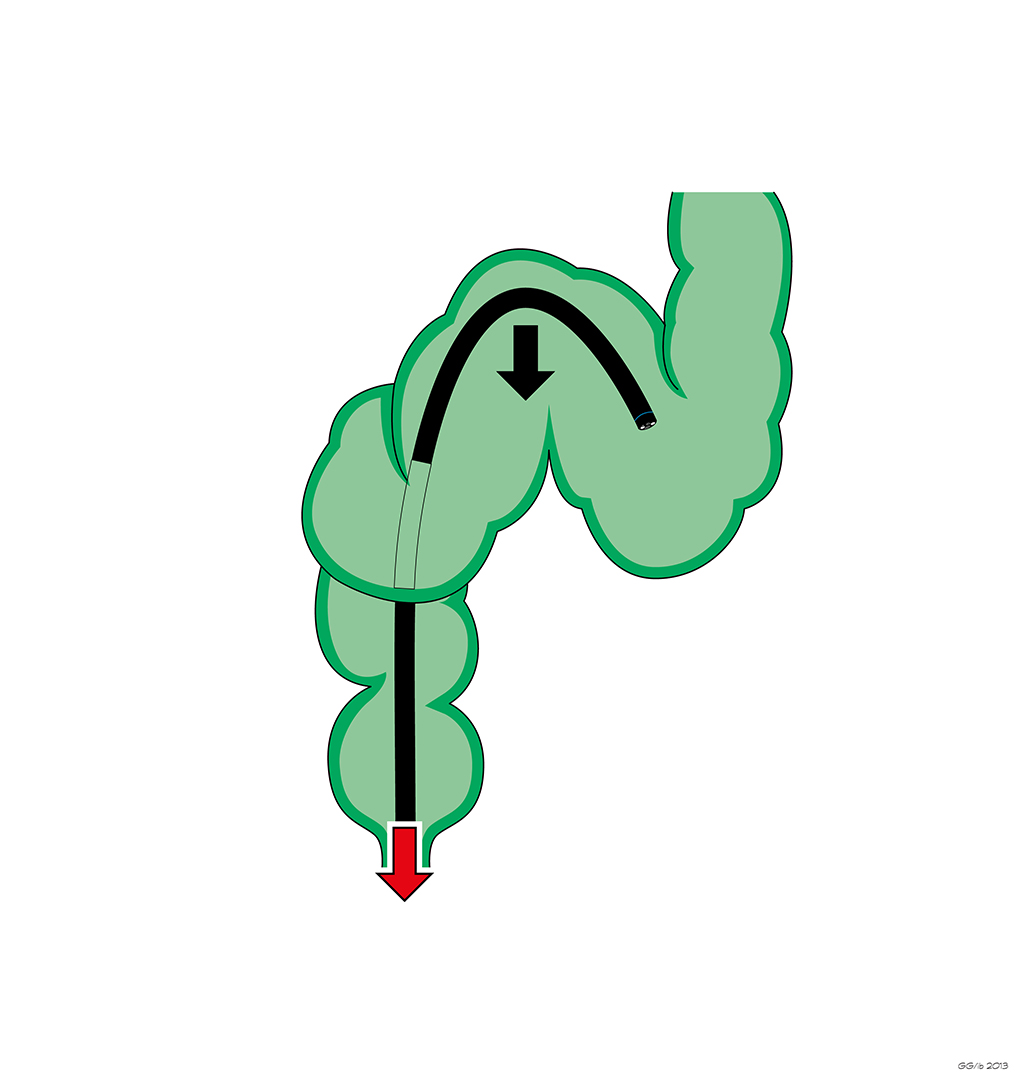

Fig. 4 A-D: The progression along a twisted loop requires maximum concentration to calibrate the advancement, that should be alternated with pull back and aspiration of air soon after having passed each loop (A-B). Besides, the endoscopist should take advantage of the rotation and angulation maneuvers (B), to straighten the loops coming in succession, and advance the scope only when he/she feels to have achieved the one-to-one effect.
If during the progression the endoscopist feels the presence of adhesions, these can be used as anchoring points, to “telescope” the distal sigmoid after intubation (Fig. 5 A-D).

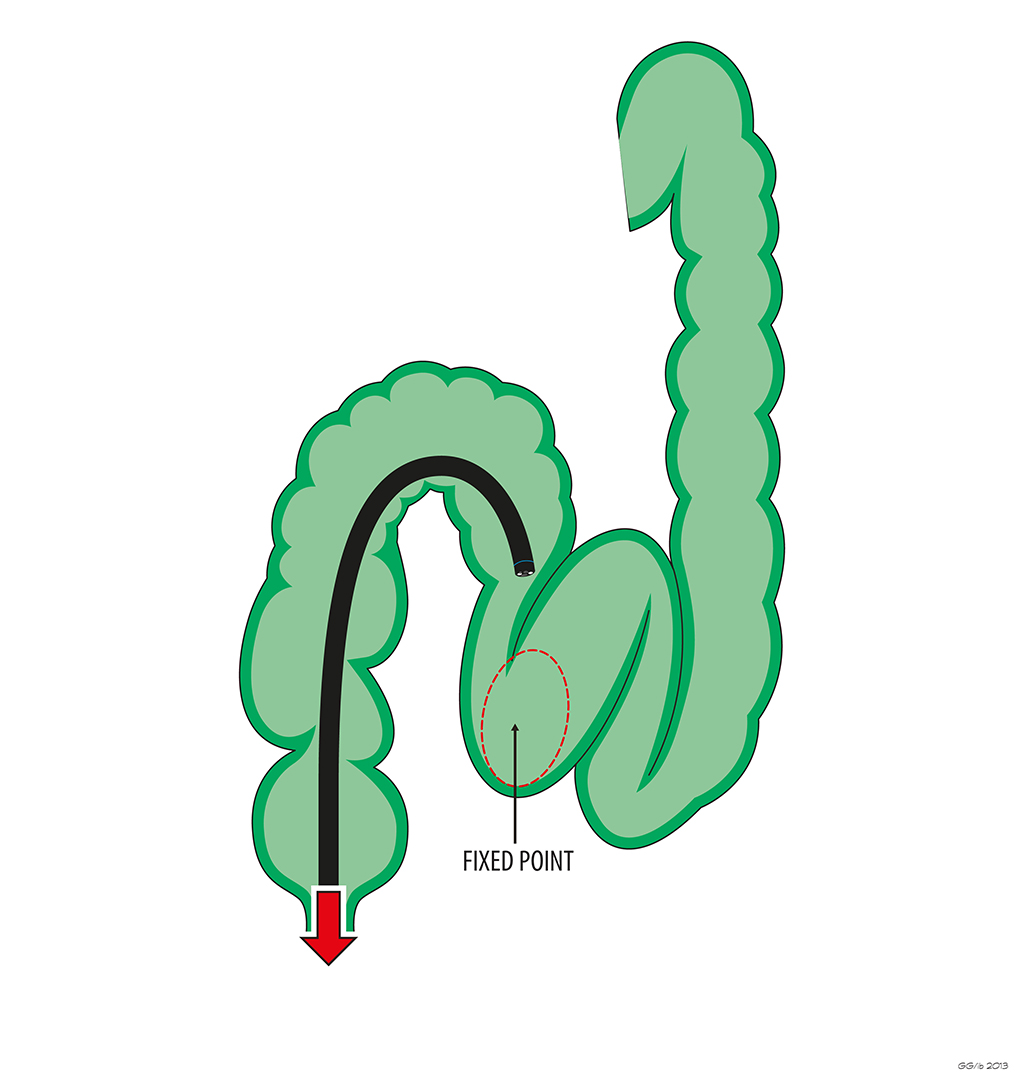
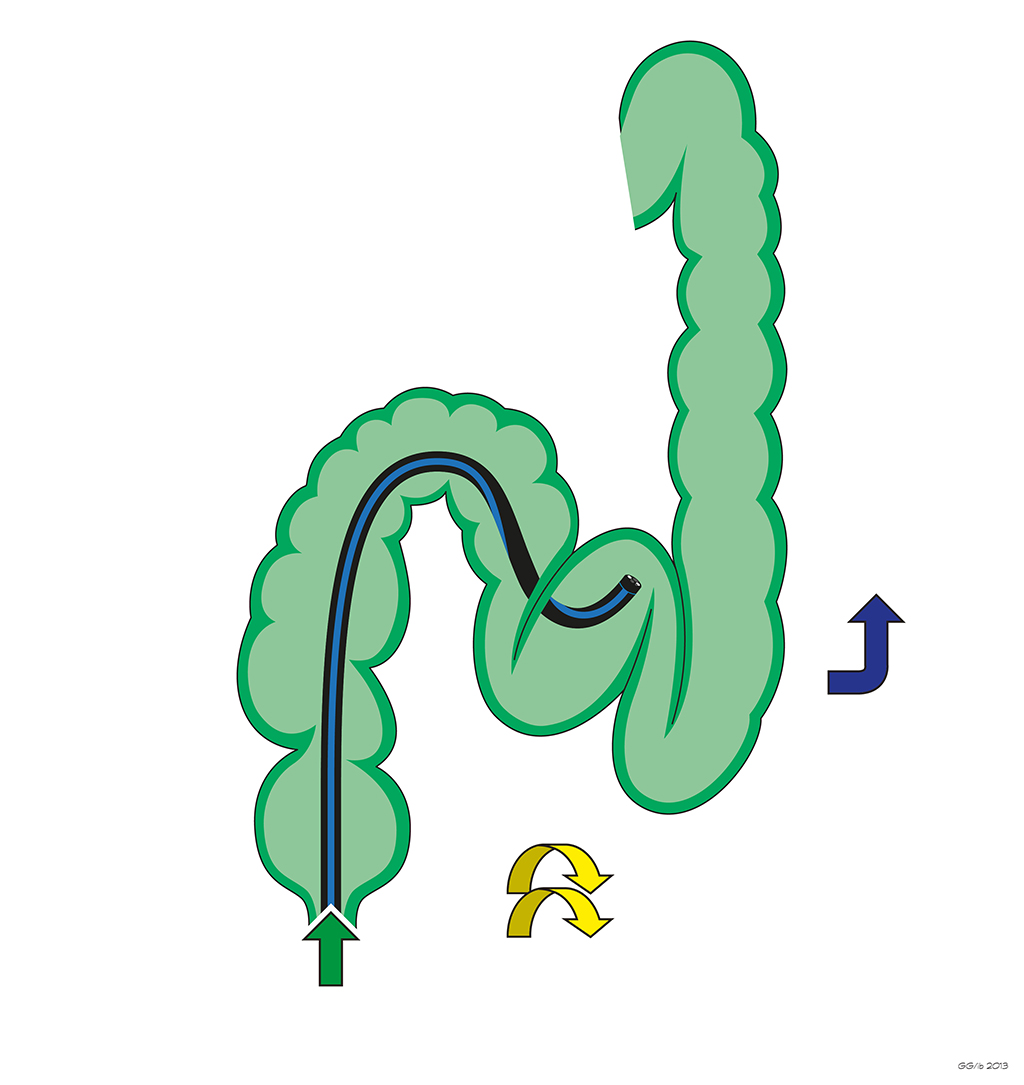

Fig. 5 A-D: the succession of advancement and pull back, together with the combination of tip deflection and shaft rotations, represent the key rules to straighten the colon and shorten the sigmoid.
When the tip of the scope approaches the sigmoido-descending junction, the endoscopist performs the maneuver to hook the fold (fig. 5 E), and then slowly and gradually pulls back the colonoscope until a resistance to the retraction is perceived; a clock-wise rotation of the shaft is made (fig. 5 F) in an attempt to reverse the residual curve.


Fig. 5 E-F: Once the sigmoido-descending junction is hooked with the tip of the scope, the colonoscope is gradually pulled back until a resistance to further retraction is perceived (4 E); then a clock-wise rotation of the shaft is made to reverse or overturn the residual curvature ( 4 F).
By the end of these maneuvers, the instrument should be positioned at the level of sigmoid-descending junction (at 30-35 cm from the anal verge) to consider the shortening effective.
Once the colonoscope has been stabilized in straight position, and the one-to-one is regained, the endoscopist can proceed with the advancement toward to splenic flexure (fig. 5 G).

Fig. 5 G: once the stabilization of the colonoscope in straight position has been verified, and the one-to-one effect regained, the endoscopist can proceed with the advancement along the descending colon.
Should the progression be awkward because of adhesions in patients with previous abdominal surgery, an alternative option is to position the patient on the right side in order to modify the opening of the recto-sigmoid angle. Further attempts in case of persistent failure due to adhesions that trap the tip of the scope, can be made using a pediatric small-caliber colonoscope or a gastroscope.
Tips for better colonoscopy from two experts – Bourke M.J. , Rex D – Am J Gastroenterol – 2012
How do I overcome Difficulties in Insertion? – Yunko J, Suck-Ho L – Clin Endosc 2012
How I teach my trainees “water navigation colonoscopy” – Mizukami T, Hibi T – Am J Clin Med - 2010